Nurse Managers were beginning to struggle, causing good people to question whether they wanted to remain in management or go back to the bedside. To keep nurse managers and other healthcare leaders, organizations must improve leadership appointment practices and development strategies that align with the complex business environment that shapes the healthcare industry.
All of this is logical. Tens of thousands of healthcare leaders fall in to the B+, B and B- levels of effectiveness. They are clearly not showing up any differently today than they were just a few short years ago. The primary contributing factor causing more leaders to struggle is the increasing complexity of management assignments. Compounding the challenges that the sudden increase in complexity poses, these are good people who are now “in over their heads.” They are not necessarily the leaders an executive might expect would need help.
Earning a B is simply not good enough anymore. Maintaining the same level of performance is effectively losing ground for B level leaders as some organizations take measures to improve, while others remain unconvinced. This is true for HCAHPS scores as much as it is true for leadership effectiveness.
Consider for a moment what is different for leaders at organizations measured as having above average performance. How do their best practices change things for nurse managers?
Primarily, these organizations achieve above average performance as a result of a disciplined and structured approach to measuring and improving leadership and management effectiveness. This requires several phases of evolution, through which best practices mature. Over time, they improve their ability to use four macro perspectives of their leader/manager’s level of effectiveness. At the above average level, politics and bias are minimized to a point of near nonexistence and the organization demonstrates a willingness and ability to identify struggling talent and use coaching to improve performance where it makes sense, or make changes to help realign the right individuals with the right roles. In every case, sophisticated Talent Management practices achieves the “Talent Shift” that defines high performance.
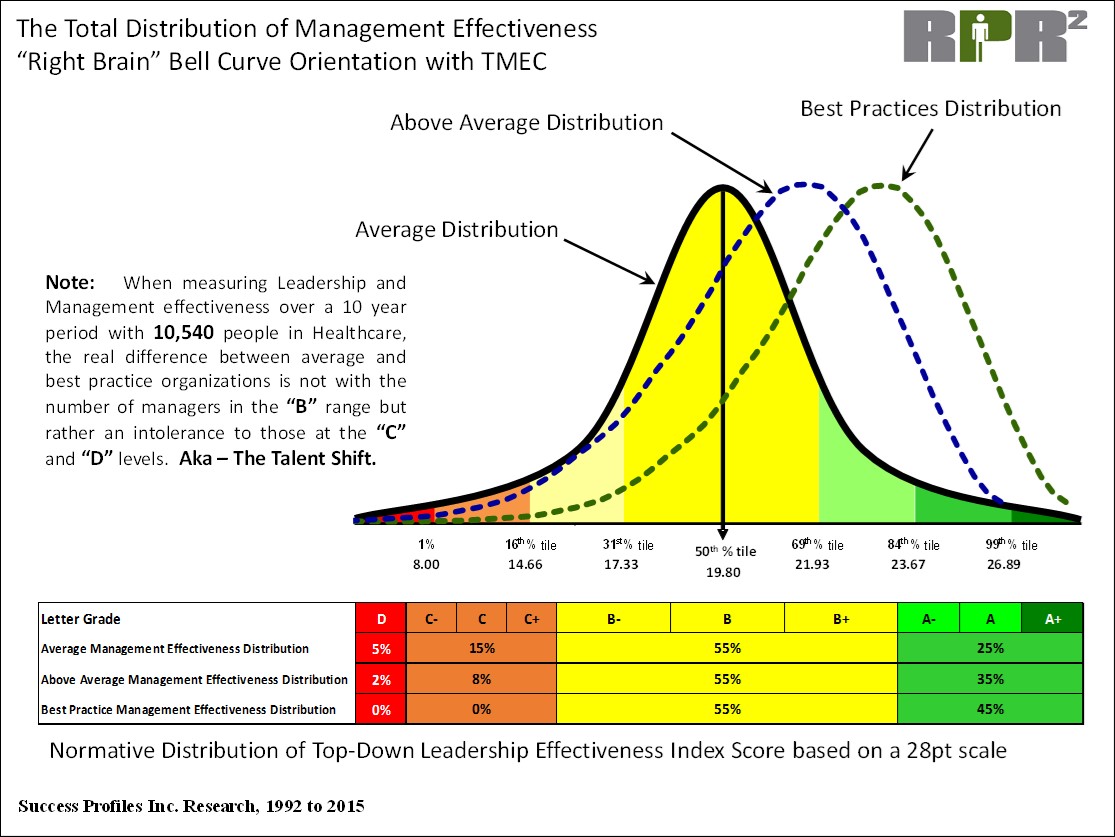
Research conducted by Success Profiles, Inc. reveals the difference. Organizations with a structured approach to Talent Management are mapped on a bell curve distribution according to management effectiveness (Chart 1). Based on the results of this research, the following conclusions can be drawn:
Below Average and Low Performing Healthcare Organizations: If the organization participated at all in measuring effectiveness, they would be skewed to the left on the bell curve distribution. But rarely do they implement a structured approach to Talent Management and therefore they have no measurable evidence of their organization’s overall leadership and management effectiveness.
Talent Management is considered a “Proactive” initiative. Because Talent Management actually requires an investment (time, resources, money), it is neglected, discounted or delayed. Healthcare executives just try to survive the incredible volume of changes to their business models.
The result is a lack of mature and sophisticated understanding of the application of business analytics. Quantifying leadership and management effectiveness is often misrepresented within the organization to be a “subjective” process.
15% of organizations do have a structured approach
Initially, most struggling leaders are long tenured “C” and “D” level managers. These are good people that were primarily appointed into management based upon tenure, experience and technical skills. 10 years ago these leaders were likely getting good results but the complexity of their job/role has gotten away from them and they are now “in over their heads.”
Executives initially struggle with the fact that these “good people,” who try hard, are not likely to turn around the performance within their span of responsibility. A number of executives will challenge the data and methodology of the Talent Management approach because “their convictions and biases are so great that they are undeterred by the evidence.”
The first phase of an improvement intervention involves immediately coaching and finding the Right Roles for the “C” and “D” level managers. This can take a few cycles because it is often difficult to replace the managers in high degree of difficulty (DoD) roles. There is eventually a significant reduction in the “C” level performers within the organization and a virtual elimination of the people at the “D” level (see table below the 3 bell curves where the number decreases from approximately 20% to 10%).
Organizations tend to struggle with the follow through process because of delays in transitioning from data collection to the coaching process. Some very vocal leaders/managers will interpret the initiative as “just another HR program” that will probably go away before it gains momentum.
The second phase involves an organization wide formal Coaching process to help those at the “B” level improve or be redeployed into more appropriate management assignments. Executives learn to avoid appointing “B’s” into High degree of difficulty roles (odds of success typically below 40%).
Management begins to appreciate the importance of emotional intelligence, behavioral style self-awareness, self-regulation and the connection to leadership effectiveness. Coaching morphs from being a legacy process that has been historically interpreted to “Fix People” to a process and skill set that is expected for everyone in management, especially for the high achievers.
The final phase involves working with the “A” level managers that represent the next generation of leaders that will assume an increased span of responsibility. The first round of leadership continuity and succession mapping is usually limited to the executives in the C-suite. The second round involves the VP’s and the third involves people in key Director roles.
There is now a widespread understanding that “C” and “D” level leaders/managers are not well suited or prepared to manage the complexity of leadership assignments. On Chart 1, the best practices bell curve distribution shows where “C’s” and “D’s” are eliminated, the total number of “B’s” stays approximately the same and the number of “A’s” increases.
There is an increased emphasis on external selection and internal appointment qualifications (and emotional intelligence) because it is much easier to help people improve that already exhibit the desired attributes of leadership/management effectiveness than to invest significant time and money in people that have a lot of heavy lifting improvements to make.
Hallmarks of a Talent Shift:
- The learning curve is accelerated by benchmarking against other successful organizations and effective leaders. Virtually every problem complexity presents has already been solved by someone else.
- Organization gets ahead of the productivity curve. Proactively makes process improvements instead of waiting for the axe to fall to cut costs (including staff).
- Leaders are good talent scouts and invest more time coaching. Average managers spend under three hours per week coaching. The ideal amount requires at least nine hours.
- Shorter leadership/management assignments become the norm.
- Clear plans for the future. The organization establishes leadership continuity plans that monitor talent “bench strengths” and adjusts for emerging development needs.
Above average and best practice organizations identify top leadership talent through a structured approach to Talent Management. It takes continuous effort to improve. Every year, the organization makes it an imperative to ratchet up leadership talent and ability to keep ahead of the increasing complexity of the healthcare leadership role. The Nurse Manager role is changing. Your talent strategy will determine whether your organization falls behind, keeps pace, or excels.
Tom Olivo, CMC, is the founding partner in the consulting firm Healthcare Performance Solutions and the president of Success Profiles, Inc. Established in 1990, Success Profiles designs and provides organizational performance measurement instruments and database management services to clients, management consulting firms and professional associations. In his professional career, Mr. Olivo has over 25 years of experience in identifying, measuring and comparing the “commonalities” of highly successful athletes, business leaders and organizations.
James Jiloty, M.S., PHR, has spent his entire career in the healthcare industry since 2003, with expertise in human resources development and leadership. He is a valued business partner to clients engaged in a structured approach to talent development and performance improvement strategy.
The views, opinions and positions expressed within these guest posts are those of the author alone and do not represent those of Becker’s Hospital Review/Becker’s Healthcare. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them.
