
To create leading healthcare institutions, physicians and hospitals must be aligned in multiple areas over a sustained period of time. However, today, the historical basis for a working relationship between physicians and hospitals has broken down due to increased competition aimed at offsetting reimbursement cuts. This breakdown, coupled with the increasing demands for quality, efficiency and coordination and the payment changes outlined in healthcare reform, has left many organizations wondering how to best rebuild physician-hospital alignment.
Recently, individual economic tools such as employment have been presented as the “silver bullet” solution, but fail to achieve full alignment. Equally misguided is the belief that communication and dialog will be enough to create a durable relationship between physicians and hospitals.
Instead, forming durable, collaborative partnerships requires the use of a variety of tools and strategies simultaneously. Given that the success of the hospital’s mission depends on physician alignment, it is incumbent on hospital administrators to define the new collaborative tenor of the relationship between hospitals and physicians and their overall alignment strategy.
As illustrated by Exhibit 1, there are three major elements required for full physician-hospital alignment.[1] 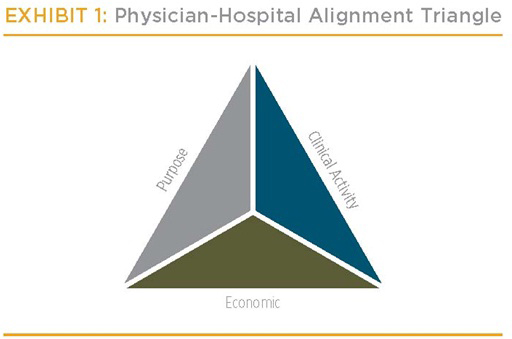 This Physician-Hospital Alignment Triangle includes:
This Physician-Hospital Alignment Triangle includes:
- Clinical Activity Alignment: The correlation of the patient care approach, expectations of quality and service, and consolidation of activity in the diagnosis, treatment and rehabilitation of a patient
- Economic Alignment: The correlation of physician and hospital financial returns
- Alignment of Purpose: The correlation of vision, values and energies; creating a shared belief in a single vision/mission, a common culture and an active involvement in the future direction of the organizations
Alignment in one area is not enough to be successful in the future environment. The future post- healthcare reform environment requires much greater integration of the continuum which in turn requires alignment on all three factors.
Unfortunately, most hospitals and healthcare systems are far from full physician alignment. To systematically study the physician-hospital alignment at hospitals and healthcare systems across the country, we developed a quantitative diagnostic tool. This tool, the Physician-Hospital Alignment Diagnostic, allows hospitals to test their specific situation and alignment against others across the country. Over a period of only a few hours per hospital, an organization can rapidly determine where it ranks on physician alignment. Evaluating the scores of hospitals for which the Physician-Hospital Alignment Diagnostic has been run demonstrates that many organizations have a significant gap in their quest for aligned and integrated physicians.
Taking a sample of 40 hospitals[2] shows some interesting results.
- The total alignment score is measured by adding the scores of the three types of alignment. With a maximum possible full alignment score of 150, the sample scores range from 59 to 106. The mean score is 81.
- Clinical activity alignment scores range from 19 to 38 of a possible 50 points with a mean score of 27
- Economic alignment scores range from 12 to 36 of a possible 50 points with a mean score of 27
- Alignment of purpose scores range from 17 to 36 of a possible 50 points with a mean score of 27
- The urgency score has a maximum of 50 points. For the sample, the measure alignment urgency range from 22 to 39 with a mean score of 30.
These scores and ranges, which are similar to other hospitals in the database, show the variability of physician-hospital alignment and that, on average, many hospitals are far from garnering the highest score in any one area.
Evaluating a sample hospital (“Hospital A”) shows a typical profile of a hospital in the database. (See Exhibit 2.) This hospital, a 200-bed hospital, has above-average financial indicators and provides strong community care to a growing, affluent, suburban market. The Physician-Hospital Alignment Diagnostic shows that Hospital A has substantially higher-than-average alignment of purpose, but average alignment in clinical activity and economic areas. Moreover, market indicators suggest that the urgency of creating stronger physician alignment is lower than average.
Further investigation of Hospital A shows that the hospital’s administration has been actively working to create a common vision with its physicians. This common vision has led to direct physician leadership in setting the strategic course of Hospital A. However, while Hospital A has kept up with the national trends, it has not been overly aggressive at using the tools that might advance clinical activity or economic alignment. For instance the Hospital A does not employ any physicians, does not pay ER call pay, and has only a very limited number of other contractual and business service activities with its physicians. Given the relatively weaker alignment within clinical activity and economic areas, Hospital A has embarked on investigating the tools that directly impact these two areas of alignment.
In contrast, another hospital in the database (“Hospital B”) is a 250-bed hospital and a sole community provider with financial and quality indicators in line with national averages. Evaluating Hospital B’s physician alignment shows a strong economic alignment, but average clinical alignment and alignment of purpose. (See Exhibit 3.) Their urgency of alignment is lower than others in the sample.
Further investigation shows this hospital uses multiple economic tools—real estate leases, strong information system connections, employment, call pay and medical directorships—to economically align physicians with the hospital. As a sole community provider in a flat market, the hospital needed to mitigate the economic threat posed by physician developing their own facilities and diagnostics to compete with the hospital. However, the tools that led to strong economic alignment did not lead to the same levels of clinical activity alignment or alignment of purpose. To further improve physician alignment Hospital B needs to deploy the specific tools targeted at clinical activity and purpose.
Tools to Improve Physician-Hospital Alignment
There are 20 major tools in four categories that hospitals can use to create the three forms of alignment. (See Exhibit 4.) The four categories each impact alignment differently.
The four categories of physician-alignment tools are not uniformly suited to drive alignment in each area (economic, clinical activity and purpose); instead, within each component of alignment, research indicates particular tool categories are more effective than others at driving alignment. Organizations wanting to improve their physician alignment in a particular area should consider deploying categories of tools according to Exhibit 5.
Within the category, hospitals should deploy tools with the appropriate degree of risk/impact for the situation. (See Exhibit 6.) High urgency scores and low physician-alignment scores indicate that higher-impact tools should be used within the appropriate category. However, because the higher-impact tools entail greater risk, if the situation does not warrant use of high-impact tools (low urgency scores and high physician-alignment scores), lower-impact tools should be deployed. The end goal is to apply the appropriate tools with the right balance of impact and risk to the create alignment.
In the case of Hospital A, the lower urgency of alignment score suggests that Hospital A should use moderate-impact tools with lower risk in the contracts and business services categories. As such, Hospital A is actively working to extend the electronic medical record to all physicians on the medical staff. Moreover, Hospital A is building off its strong alignment of purpose to create a clinical integrated physician network for better care coordination and allowing the physicians and hospital to contract together. Additionally, medical directorships are being reevaluated to ensure they advance the vision of the hospital’s operations and a clinical co-management relationship in cardiology is under development.
In contrast, Hospital B, with lower clinical activity alignment and alignment of purpose, would do well to focus efforts on redefining contracts (e.g., medical directorships) to focus on quality, safety and operational improvement metrics to advance the clinical activity position and create a wide range of structured communications tools to create a common sense of purpose.
While our diagnostic has shown that the level of physician-hospital alignment varies between hospitals, it is clear that most hospitals have the potential for significant improvement in at least one alignment area. Moreover, there is not one tool that will single handedly address all three areas requiring alignment. As physician-hospital alignment and integration become increasingly important to delivering quality and efficient care, it is essential to understand how your organization compares to peer organizations and how to increase alignment in your specific situation. Start this process at www.PhysicianHospitalAlignment.com by taking a free version of the diagnostic and discovering your organization’s performance and steps for improvement.
Kate Lovrien is a senior strategy manager from Kurt Salmon’s Minneapolis office. She has focused her career on advising community and regional referral hospitals and healthcare systems on their strategic and physician alignment challenges. Kate is the lead author of the Physician-Hospital Alignment Diagnostic located at www.PhysicianHospitalAlignment.com. She can be reached at 612.865.6088 or Kate.Lovrien@kurtsalmon.com.
Luke Peterson is a strategy partner from Kurt Salmon’s Minneapolis office. He has focused his career on advising community and regional referral hospitals and healthcare systems particularly on the physician-hospital relationships and healthcare system organizational structures and roles. He can be reached at 612.810.8188 or at Luke.Peterson@kurtsalmon.com.
[1] For a more thorough treatment of the topic of physician-hospital relationships, read Kurt Salmon’s paper titled Physician-Hospital Alignment at www.kurtsalmon.com
[2] The 40 hospitals were chosen to provide a cross section of the typical community hospital in the U.S. today. These hospitals all depend heavily on a private practice medical staff, are located in urban and suburban markets and range from 150 to over 500 beds. These hospitals represent typically high-quality, successful organizations.![]() Kurt Salmon is the premier management consulting firm for today’s leading hospitals and health systems. We work closely with our clients to create tailored solutions for their strategic and finance, facility development and performance, operational and information technology needs. In the past three years, we have worked with all of U.S. News’ Top Hospitals.
Kurt Salmon is the premier management consulting firm for today’s leading hospitals and health systems. We work closely with our clients to create tailored solutions for their strategic and finance, facility development and performance, operational and information technology needs. In the past three years, we have worked with all of U.S. News’ Top Hospitals.
_________________________________________________________________________________________________________________________________________________________________________________________