Respiratory depression has been associated with the use of opioid analgesics. However, a recent study by researchers at Wesley Medical Center in Wichita, Kan., suggests exhaled CO2 monitoring of patients using patient-controlled analgesia pumps could help reduce the occurrence of this adverse event. Specifically, Debra Fox, MBA, RRT-NPS, and Mark Wencel, MD, examined respiratory depression rates with the use of PCA pumps and intermittent IV opioids for pain management.[1]
Respiratory depression is an identified patient safety issue. As The Joint Commission recently stated in its Sentinel Event Alert, "Safe Use of Opioids in Hospitals:"
"Opioid analgesia may result in unrecognized or at least unattributed deaths. The risk of patient deaths from PCA prompted Wesley to invest in 'smart' pump technology with integrated capnography. We are strong advocates for end tidal CO2 measurement with capnography over the sometimes suggested pulse oximetry," explained Ms. Fox.
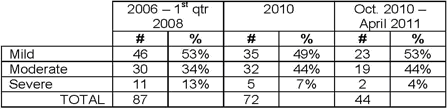
The chart below reflects the impact of the initiative. As the chart demonstrates, the percentage of severe ADRs drops from 13 percent to 4 percent, or threefold, following the integration of capnography with smart pumps. "This drop may be attributed to earlier recognition of respiratory depression," says Dr. Wencel.
To achieve this reduction in severity, the team identified patients who were most exposed to experiencing an adverse drug event. "We implemented a high-risk screening process that issued scores according to the STOP BANG model for obstructive sleep apnea," says Ms. Fox, who helped design the program. "The screening process incorporated additional risk factors for respiratory depression into patients' personal health history." Doing so required respiratory care to develop and provide education on end tidal CO2 monitoring for all staff and physicians.
The guide shows that well-structured systems enable healthcare professionals to break down silos and treat patients safely in a timely manner.
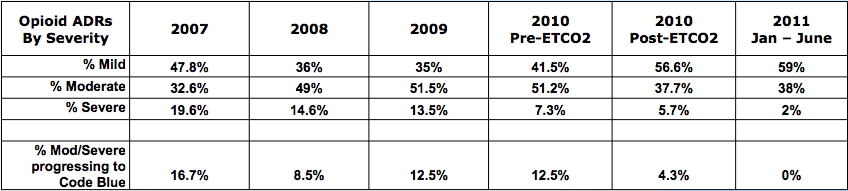
Dr. Wencel adds, "The percentage of moderate and severe ADRs progressing to code blue fell from just under 13 percent to just over 4 percent. Through the first half of 2011, that progression rate sat at 0 percent."

"Equally important, our study highlights the positive impact that multidisciplinary teams can have on patient safety with well crafted policies and procedures," notes Dr. Wencel. "When healthcare units work together on implementing initiatives such as smart pumps with integrated capnography, the patient benefits."
More recent results at the hospital are so encouraging that Wesley Medical Center is planning to expand the monitoring program. "Our latest results show the sustained reduction in our severe ADRs," explains Ms. Fox. "The hospital's safe medication practice committee is now considering expanding ETCO2 monitoring to all patients receiving intermittent IV opioids, not just those that score as a high risk."
Footnotes:
[1] The study appeared as an abstract and poster presentation in 2011 for the American Association for Respiratory Care.
Michael Wong is founder and executive director of the Physician-Patient Alliance for Health & Safety. Passionate about patient safety, he was recently invited by the American Board of Physician Specialties to be a founding member of the American Board of Patient Safety. He is a graduate of Johns Hopkins University and is on the editorial board of the Journal of Patient Compliance, a peer-reviewed journal devoted to improving patient adherence.
Sean Power is the Community Manager for the Physician-Patient Alliance for Health and Safety. He also blogs for a non-profit medical and research foundation, AMREF, that focuses on improving healthcare in Africa. Power cares deeply about achieving better clinical outcomes for all patients in every healthcare facility.
Respiratory depression is an identified patient safety issue. As The Joint Commission recently stated in its Sentinel Event Alert, "Safe Use of Opioids in Hospitals:"
While opioid use is generally safe for most patients, opioid analgesics may be associated with adverse effects, the most serious effect being respiratory depression, which is generally preceded by sedation.
Integrated capnography detects respiratory depression early
The Joint Commission, the American Society of Anesthesiologists and the Institute for Safe Medication Practices recommend the monitoring of exhaled CO2 to detect respiratory depression to increase patient safety with pain medication administration. Consequently, the Wesley Medical Center converted to a "smart" infusion pump system with integrated capnography. These smart pumps monitored levels of exhaled CO2, thereby detecting a potential adverse drug event and respiratory depression early on."Opioid analgesia may result in unrecognized or at least unattributed deaths. The risk of patient deaths from PCA prompted Wesley to invest in 'smart' pump technology with integrated capnography. We are strong advocates for end tidal CO2 measurement with capnography over the sometimes suggested pulse oximetry," explained Ms. Fox.
How the Wesley Medical Center implemented the initiative for patients on opioid pain management programs
In 2010 the Wesley Medical Center decided to develop a safe pain management program and formed a multidisciplinary team of providers to oversee its implementation, explains Dr. Wencel, who worked on the project. "We formed a multidisciplinary team made up professionals from respiratory care, pharmacy, anesthesia and nursing. We included key physicians who collaborated on hospital-wide policies and procedures. Involving multiple stakeholders within the hospital meant that new processes received buy-in from key people," he says.The chart below reflects the impact of the initiative. As the chart demonstrates, the percentage of severe ADRs drops from 13 percent to 4 percent, or threefold, following the integration of capnography with smart pumps. "This drop may be attributed to earlier recognition of respiratory depression," says Dr. Wencel.
To achieve this reduction in severity, the team identified patients who were most exposed to experiencing an adverse drug event. "We implemented a high-risk screening process that issued scores according to the STOP BANG model for obstructive sleep apnea," says Ms. Fox, who helped design the program. "The screening process incorporated additional risk factors for respiratory depression into patients' personal health history." Doing so required respiratory care to develop and provide education on end tidal CO2 monitoring for all staff and physicians.
Improving patient safety through RT/RN bedside collaboration
The team implemented procedures for responding to alarm situations that involved respiratory therapists and registered nurses. Below is the step-by-step process now being followed at Wesley Medical Center:- RN notifies RT of alarm situation
- Patient assessment
- Sedation scale
- Respiratory rate and tidal volume
- Confirm correct placement of sampling cannula
- Stimulate patient to take deep breaths if necessary
- Collaborate to review pain medication orders
- Contact physician
- Naloxone reversal if indicated
- RT may initiate non-invasive ventilation
- BiPAP (IPAP 15, EPAP 5, Rate 12)
- Continue ET CO2 monitoring with non-invasive ventilation.
- Follow-up call to physician after one hour if ventilatory assistance is still needed. Consider transfer to ICU.
The guide shows that well-structured systems enable healthcare professionals to break down silos and treat patients safely in a timely manner.
Impact of end tidal CO2 monitoring
The chart below shows a decline in the incidence of severe adverse drug events involving PCA. "Since implementing the smart infusion pump system with integrated capnography the incidence of severe ADRs has fallen to below 5 percent. Just three years ago the figure was three times that rate," says Ms. Fox.Dr. Wencel adds, "The percentage of moderate and severe ADRs progressing to code blue fell from just under 13 percent to just over 4 percent. Through the first half of 2011, that progression rate sat at 0 percent."
Integrated capnography makes pain management programs safer for the patient
According to the study, continuous electronic monitoring of ventilation and oxygenation is correlated with improved safety for patients on opioid pain management programs. "Our study demonstrates that the use of end-tidal CO2 monitoring is an effective method for early detection of respiratory depression in patients receiving PCA and intermittent IV opioid pain medication," says Ms. Fox."Equally important, our study highlights the positive impact that multidisciplinary teams can have on patient safety with well crafted policies and procedures," notes Dr. Wencel. "When healthcare units work together on implementing initiatives such as smart pumps with integrated capnography, the patient benefits."
More recent results at the hospital are so encouraging that Wesley Medical Center is planning to expand the monitoring program. "Our latest results show the sustained reduction in our severe ADRs," explains Ms. Fox. "The hospital's safe medication practice committee is now considering expanding ETCO2 monitoring to all patients receiving intermittent IV opioids, not just those that score as a high risk."
Footnotes:
[1] The study appeared as an abstract and poster presentation in 2011 for the American Association for Respiratory Care.
Michael Wong is founder and executive director of the Physician-Patient Alliance for Health & Safety. Passionate about patient safety, he was recently invited by the American Board of Physician Specialties to be a founding member of the American Board of Patient Safety. He is a graduate of Johns Hopkins University and is on the editorial board of the Journal of Patient Compliance, a peer-reviewed journal devoted to improving patient adherence.
Sean Power is the Community Manager for the Physician-Patient Alliance for Health and Safety. He also blogs for a non-profit medical and research foundation, AMREF, that focuses on improving healthcare in Africa. Power cares deeply about achieving better clinical outcomes for all patients in every healthcare facility.